PDF-POLICY APPLICATION (please print or type)
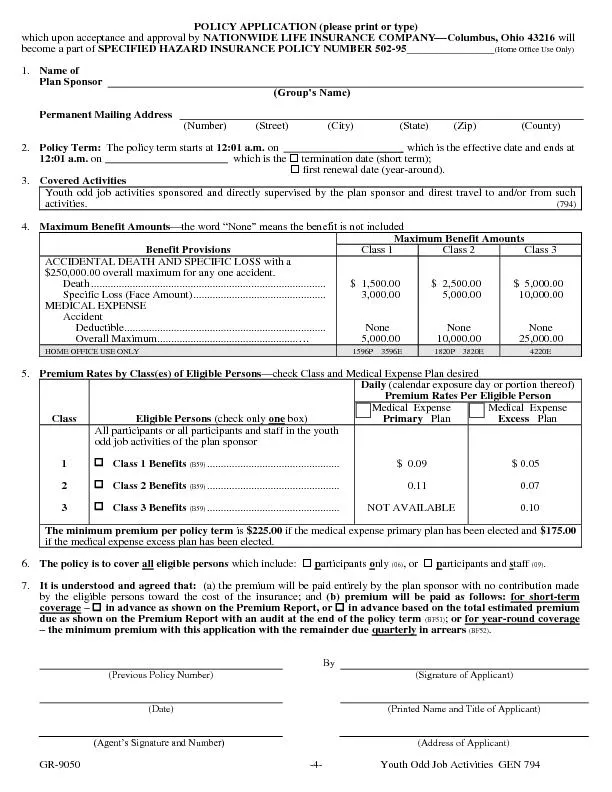
which upon acceptance and approval by NATIONWIDE LIFE INSURANCE COMPANY
xF0BE
Columbus Ohio 43216
will become a part of SPECIFIED HAZARD INSURANCE POLICY NUMBER
Download Presentation
"POLICY APPLICATION (please print or type)" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.