PDF-Journal of Clinical and Diagnostic Research. 2011 November (Suppl-2),
Author : cheryl-pisano | Published Date : 2015-10-15
1461 1461 A Rare Case of Pregnancy in the Rudimentary Horn of Unicornuate Uterus on Table Diagnosis Which had a Key Wor DHANANJAYA BS SHOAGOPAL K Case Report was
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Journal of Clinical and Diagnostic Resea..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Journal of Clinical and Diagnostic Research. 2011 November (Suppl-2),: Transcript
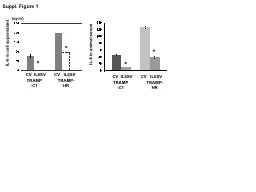
1461 1461 A Rare Case of Pregnancy in the Rudimentary Horn of Unicornuate Uterus on Table Diagnosis Which had a Key Wor DHANANJAYA BS SHOAGOPAL K Case Report was 106gdl her RBS was 98mgdl u. INDIAN J MED RES (SUPPL) MAY 2004sinusitis). Gram stained smears and cultures were group were further tested for ATCC 49619 was used for quality atmosphere, except for erythromycin andclindamycin when INDIAN J MED RES (SUPPL) MAY 2004 2006 J. Neurosurg: Pediatrics / Volume 105 / November, 2006 1914 Dandy and Blackfan described a congenitalmalformation of the central nervous system comprisingdilation of the fourth ventricle, hypopla IL-6 in cell supernatant. IL-6 in animal serum. TRAMP-C1. TRAMP-HR. CV IL6SV CV IL6SV. TRAMP-C1. TRAMP-HR. CV IL6SV CV IL6SV. (. ng. /ml). *. *. *. *. IHC CD31. TRAMP-C1. TRAMP-HR. to Wrongness. John Banja, PhD. Center For Ethics. Emory University. jbanja@emory.edu. Why Be Interested in Diagnostic Error?. Diagnostic errors are the leading cause of medical malpractice suits: 45% of cases. Gene expression changes in cationic channels, free radical/antioxidant pathways and vesicular transport proteins induced by bacterial . LPS+IFNγ. stimulation in hEGC. . Box plots of mRNA counts/100ng sample showing differences in gene expression between control (CON, unstimulated) and LPS (stimulated) samples of hEGC (n=12-16 samples of hEGC obtained from GI surgical specimens of 4 human subjects). . Progress in . backreaction. Syksy Räsänen. University of Helsinki. Department of Physics. . and. The Helsinki Institute of Physics. 1. IAP workshop, November 22, 2011. Looking for a factor of 2. Homogeneous and isotropic models which have ordinary matter and gravity disagree with cosmological observations by a factor of 2.. 13241324ID JCDR/2012/41082448Travellers Health Through 147EmporiatricsKey Words Travel medicine Travelers health Travel hazards ABSTRACT147Travel broadens the mind148 and people have been extolling 1281 Burkholderia cepacia - An unusual organism for sepsis in ICUs. Key WorImmuno -competent, ICU sepsis, Burkholderia cepacia, BACTEC culture.ICU sepsis is a common situation encountered in practice Articles FromtheClinicalResearch,Investigation,andSys-temsModelingofAcuteIllness(CRISMA)Laboratory,DepartmentofCriticalCareMedicine,UniversityofPittsburghSchoolofMedicine,Pittsburgh,United variableand Hymenolepis. nana. Authors: Javier Gutierrez Jimenez, J.A. Hernandez-. Shilon. , L.P. Fajardo-Martinez, Maria Guadalupe del Carmen Torres-Sanchez. Citation: Javier Gutierrez Jimenez, J.A. Hernandez-. WHAT IS EVIDENCE - BASED MEDICINE (EBM)?. The translation of medical research into clinical practice. Integration of best research evidence with clinical experience and patient values. Knowing how to use clinical literature to ensure optimal patient care. Mirella Fraquelli. Gastroenterology and Endoscopy Unit. Fondazione IRCCS Ca’ Granda . Ospedale Maggiore Policlinico - Milan. DIAGNOSIS: the pathway of a diagnostic test from bench to bedside. Basic residential course.
Download Rules Of Document
"Journal of Clinical and Diagnostic Research. 2011 November (Suppl-2),"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents