PPT-Nerve Injuries of the U
Author : evans | Published Date : 2023-05-23
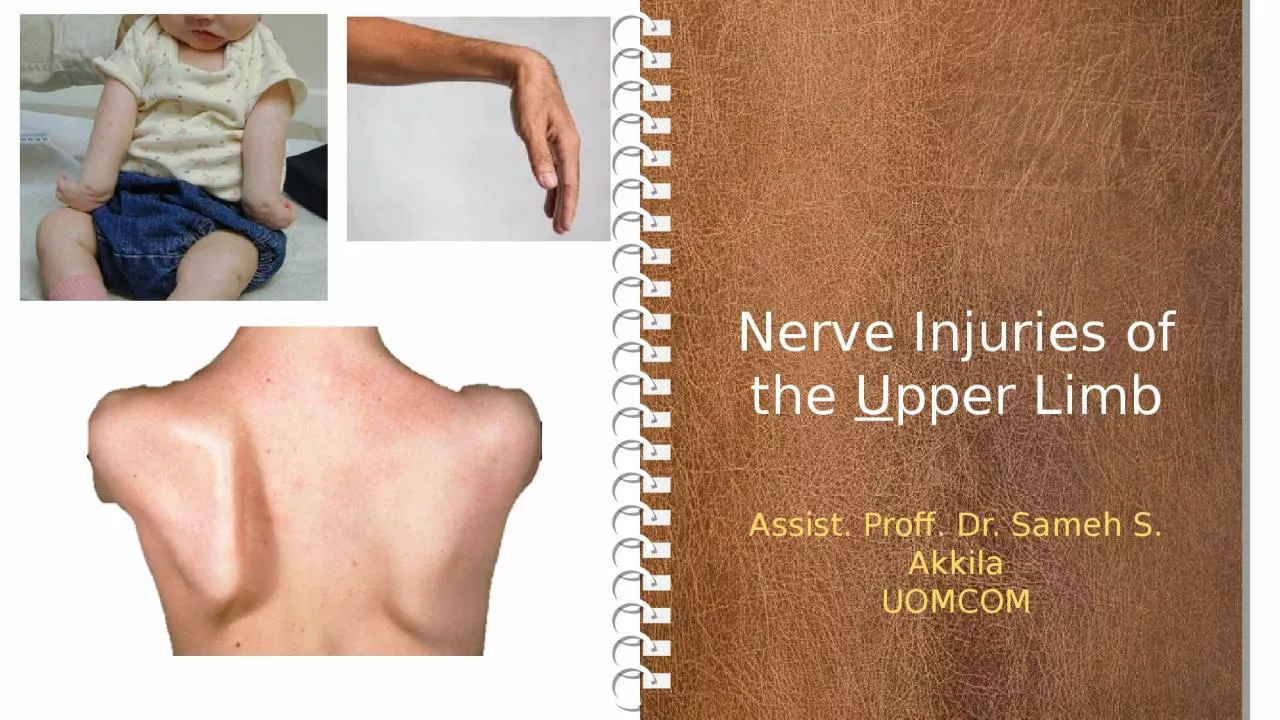
pper Limb Assist Proff Dr Sameh S Akkila UOMCOM Objectives Why How 1 Understand why nerve injuries of the upper limb are common amp important 2 Classify the types
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Nerve Injuries of the U" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Nerve Injuries of the U: Transcript
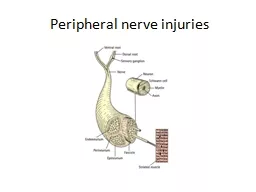
pper Limb Assist Proff Dr Sameh S Akkila UOMCOM Objectives Why How 1 Understand why nerve injuries of the upper limb are common amp important 2 Classify the types of nerve injuries amp the different outcomes of each. 500 G. S HANKAR G ANESH , D EMONSTRATOR , P HYSIOTHERAPY Nerve injuries are quite common and may have serious implications for the patient. Most nerve injuries result from either acute injury or chr Dr. Eranda Epaarachchi . The layers of the skin . Anatomy of the skin . Classification of burns – . By depth . What is shown here?. What is the diagnosis?. First degree burns . Characteristics . Epidermis is involved . Dr. Richard Bwana Ombachi. Lecturer and Consultant Spine & Orthopaedic surgeon . Introduction. Spine -Vertebral Column/Nervous Tissue. 5% worsen in the hospital. Protection is priority –Diagnosis a secondary priority. &. r. educing risk of fire. . 1. Unintentional . injuries . leading cause of preventable death for under 5s. Major cause of ill health and serious disability. 102 children & young people died annually between 2008 – 2012. Chapter 12. Injuries to the Extremities. The extremities consist of—. Bones.. Soft tissue.. Blood vessels.. Nerves.. Signals of an injury. Pain or tenderness.. Swelling.. Discoloration.. Deformity of the limb.. Firefighter I. Copyright . and Terms of Service. Copyright © Texas Education Agency, 2011. . These m. aterials. are copyrighted © and trademarked ™ as the property of the Texas Education Agency (TEA) and may not be reproduced without the express written permission of TEA, except under the following conditions:. Alistair Ross MB FRCS. Consultant Orthopaedic Surgeon, Bath, UK. Associate Editor. The Bone & Joint Journal. Cambridge Annual Medico-Legal Conference . Peterhouse,Cambridge,2016. Peripheral nerve: organisation. NERVE STRUCTURE AND FUNCTION. Peripheral . nerves are bundles of axons conducting. efferent (motor) impulses from cells in the anterior. horn of the spinal cord to the muscles, and afferent. (sensory) impulses from peripheral receptors via cells. Since the chest, abdomen, and pelvis contain many organs important to life, injury to these areas can be fatal.. . Chest injuries are a leading cause of trauma deaths each year.. Common types of injuries include rib fractures and puncture wounds.. La gamme de thé MORPHEE vise toute générations recherchant le sommeil paisible tant désiré et non procuré par tout types de médicaments. Essentiellement composé de feuille de morphine, ce thé vous assurera d’un rétablissement digne d’un voyage sur . SYNOPSIS. INTRODUCTION. NERVE INJURIES. ANATOMY OF LINGUAL NERVE. FUNCTIONS OF LINGUAL NERVE. LINGUAL NERVE INJURY. ETIOLOGY. PATHOPHYSIOLOGY. PREDISPOSING FACTORS. SIGNS AND SYMPTOMS. EXAMINATION. DIAGNOSIS-IMAGING. The roots, trunks, and divisions of the brachial plexus reside in the lower part of the posterior triangle of the neck. whereas the cords and most of the branches of the plexus lie in the . axilla. Complete lesions involving all the roots of the plexus are rare. outline. Definition. Incidence. Risk Factors. Types of Birth Injuries. Approach to a neonate with birth trauma. Investigations . Definition . Birth injuries are injuries that occur during the birth process. Done by: . Amer. Al-. Salamat. Objectives. Classification . and pathology. Upper limb- Brachial Plexus Injuries, . Erbs. Palsy, median nerve . injuries, . Unlnar. . Nerve injuries, Radial Nerve .
Download Document
Here is the link to download the presentation.
"Nerve Injuries of the U"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents