PDF-THE PUBLISHING HOUSE MEDICINE OF THE ROMANIAN ACADEMY
Author : giovanna-bartolotta | Published Date : 2016-07-15
Research article TYPE 2 DIABETES
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "THE PUBLISHING HOUSE MEDICINE OF ..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
THE PUBLISHING HOUSE MEDICINE OF THE ROMANIAN ACADEMY: Transcript
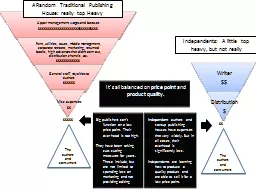
Research article TYPE 2 DIABETES. 25-9-2013- 31-10- 2013. ROMANIA. Cluj. . Napoca. ROMANIA. Romania, in southeast Europe, is mountainous in the north while the main feature in the south is the vast Danube valley. The river forms a delta as it approaches the Black Sea, which is a wildlife reserve for countless native and migratory birds.. Walter Starkie, Raggle-Taggle, 1933. ROMANIA. It came into being when the two principalities of Moldavia and Wallachia broke the shackles of Turkish Ottoman suzerainty and merged, in 1859, to form a new land - ‘Romania. It’s all balanced on . price point . and . product quality.. $$$$$. $$. B. ig publishers can’t function on a low price point. Their over head is too high. . T. hey have been taking cuts cutting measures for years. These include, but are not limited to spending less on marketing and not providing editing . Maritime Safety and Security II. . Seminar on the Implementation of measures to ensure that safety standards are ’’to the satisfaction of the Administration’’. Istanbul. , . Turkey. , . Răzvan Trandafir – Technical Director. November 2012 Istanbul, Turkey. C. . Neagoe. , L.M. . Manea. and C. Ionescu. National Institute for Earth Physics, . Magurele-Ilfov. , Romania. . In . February 1977, the Department of Seismology from the Romanian Geophysical and Geological Institute (GGI) together with the Laboratory of Geodynamics of the Romanian Academy formed the Centre of the Earth Physics (CEP). In 1994, after a governmental decision, CEP was transformed in the National Institute for Earth Physics (NIEP). NIEP is coordinated by the Romanian Ministry of Education, Research, Youth and Sport. . By Nathalie, Rachel M and Joanna. . This is our project on Romania. We really enjoyed learning about Romania. We hope you learn as much as we did and enjoy this project. . INTRODUCTION. . PHYSICAL. RELIGIOUS TRADITIONS. The . N. ational Holidays from Romania. . COMENIUS. . MULTILATERAL PROJECT . 2013-2015. Nr. LLP Link: 2013-1-PL1-COM06-38866 2. Disclaimer. This project has been funded with support from the European Commission. The presentation reflects the views only of the author, and. Romanian orphan studies. Attachment – Lesson 10. Recap task. Outline Bowlby’s Maternal Deprivation Hypothesis. Describe one study to support this. Provide two evaluation points of his theory. Effects . Teodora . Popescu. University of Alba Iulia, Romania. 1. 6. -. 6. 8. . June . 201. 7. , . Alba Iulia. Introduction. Main research project:. Universals and variants of English and Romanian business metaphors. A corpus-based conceptual mapping of . La gamme de thé MORPHEE vise toute générations recherchant le sommeil paisible tant désiré et non procuré par tout types de médicaments. Essentiellement composé de feuille de morphine, ce thé vous assurera d’un rétablissement digne d’un voyage sur . Eminescu. 1884. Mihai . Eminescu. . (1850 - 1889) . is . regarded as the greatest and the most famous Romanian poet. His life, work and poetry strongly influenced the Romanian culture. . His . poems are widely studied in Romanian schools and have been translated in over 60 languages.. Famous Romanian . minority . sportspeople. Liceul Teoretic Gheorghe Munteanu Murgoci. Gabriela Bucur. Janina . Izabela Mihai . What. . does. . bullying. . mean. ?. Bullying. . is. a . form. of . Regional Challenges: A Romanian Perspective Thursday, April 3, 2008 1:00 pm to 2:30 pm Hoover Building, Room 100 Prince Radu is visiting the Bay Area as special representative of the Romanian gov Major General Ret Leonardo Dinu is a member of the Scientific Council within New Strategy Center He retired as a two-star generalin the Romanian Army after nearly 38-year career as deputy chief of Rom
Download Document
Here is the link to download the presentation.
"THE PUBLISHING HOUSE MEDICINE OF THE ROMANIAN ACADEMY"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents