PPT-Erythropoiesis and general aspects of
Author : hadly | Published Date : 2023-05-27
anaemia AssistProf DrMaysem M Alwash Erythropoiesis is the generation of red blood cells All the circulating blood cells derive from pluripotential stem
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Erythropoiesis and general aspects of" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Erythropoiesis and general aspects of: Transcript
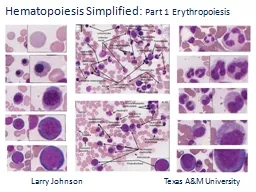
anaemia AssistProf DrMaysem M Alwash Erythropoiesis is the generation of red blood cells All the circulating blood cells derive from pluripotential stem cells in the marrow. unless otherwise specified Particulars Standard Charges NRE NRO NRE NRO NRE NRO Saving Ac PINS Ac Current Ac AVERAGE QUARTERLY BALANCE AQB NA 10000 Nil 25000 REMITTANCE Not allowed for nonbroker third party transactions DD at branch location pa a . new framework for student . reflection. Rachel Lofthouse & Roger Knill,. School of Education, Communication & Language . Sciences. ,. Newcastle . University. TEAN Conference . 21. st. M. of . Modern Cryptography. Josh Benaloh. Brian . LaMacchia. Winter 2011. Agenda. Guest lecture. Final project presentation logistics. The Politics of Crypto. Export Controls. Key Escrow. The Clipper Chip. William Empson, PE, PMP . Senior Levee Safety Program Risk Manager. U.S. Army Corps of Engineers. Risk Management Center . William.B.Empson@usace.army.mil. Dam Safety Workshop. Brasília, Brazil. 20-24 May 2013. of . Modern Cryptography. Josh Benaloh. Brian . LaMacchia. Winter 2011. Some Tools We’ve Developed. Homomorphic Encryption. Secret . Sharing. Verifiable Secret Sharing. Threshold Encryption. By Kendall and Mitchell. What an introvert is:. An introvert is someone who loses energy in social interactions, and feels re-energized while in solitude. Their social circles are condensed. They’re content with having a fewer amount of friends. . of . Modern Cryptography. Josh Benaloh. Brian . LaMacchia. Winter 2011. January 6, 2011. Practical Aspects of Modern Cryptography. Cryptography is .... Protecting Privacy of Data. Authentication of Identities. a . new framework for student . reflection. Rachel Lofthouse & Roger Knill,. School of Education, Communication & Language . Sciences. ,. Newcastle . University. TEAN Conference . 21. st. M. Josh Benaloh. Tolga Acar. Fall 2016. October 25, 2016. 2. The wiretap channel. Key (K. 1. ). Key (K. 2. ). Eavesdropper. Plaintext. (P). Noisy insecure. channel. Encrypt. Decrypt. Alice. Bob. Plaintext. Part 1 Erythropoiesis. . . . Larry Johnson Texas A&M University. Hematopoiesis . Simplified: . Part . 1 Erythropoiesis. . Objectives are to:. Identify the developmental . and . Hb. synthesis. Dr. Sunita Mittal. Learning Objectives. ▪. Factors affecting erythropoiesis. ▪. Hemoglobin synthesis. Factors regulating Erythropoiesis. Φ. . Growth or Developmental Factors. Learning Objectives. Stem cells. Process of . e. rythropoiesis -. . site, stages. Factors affecting erythropoiesis. Hematopoiesis. The process of formation of new blood cells. 4. ▫ . Blood (. Hemopoietic. ". Regulatory and Procedural Barriers to Trade in Kyrgyzstan: Needs Assessment. ". Jan Bohanes. Senior Counsel, Advisory Centre on WTO Law. Geneva, 1 September 2015. Overview of selected topics. Regulatory and . pluripotent stem cells . in the marrow. . They divide into three main types.. Erythropoiesis. , is formation of RBC. Leucopoiesis . (myelopoiesis) is formation of WBC. Thrombopoiesis. is formation of platelets..
Download Document
Here is the link to download the presentation.
"Erythropoiesis and general aspects of"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents