PDF-Refer to Form DR700025 before completing this form
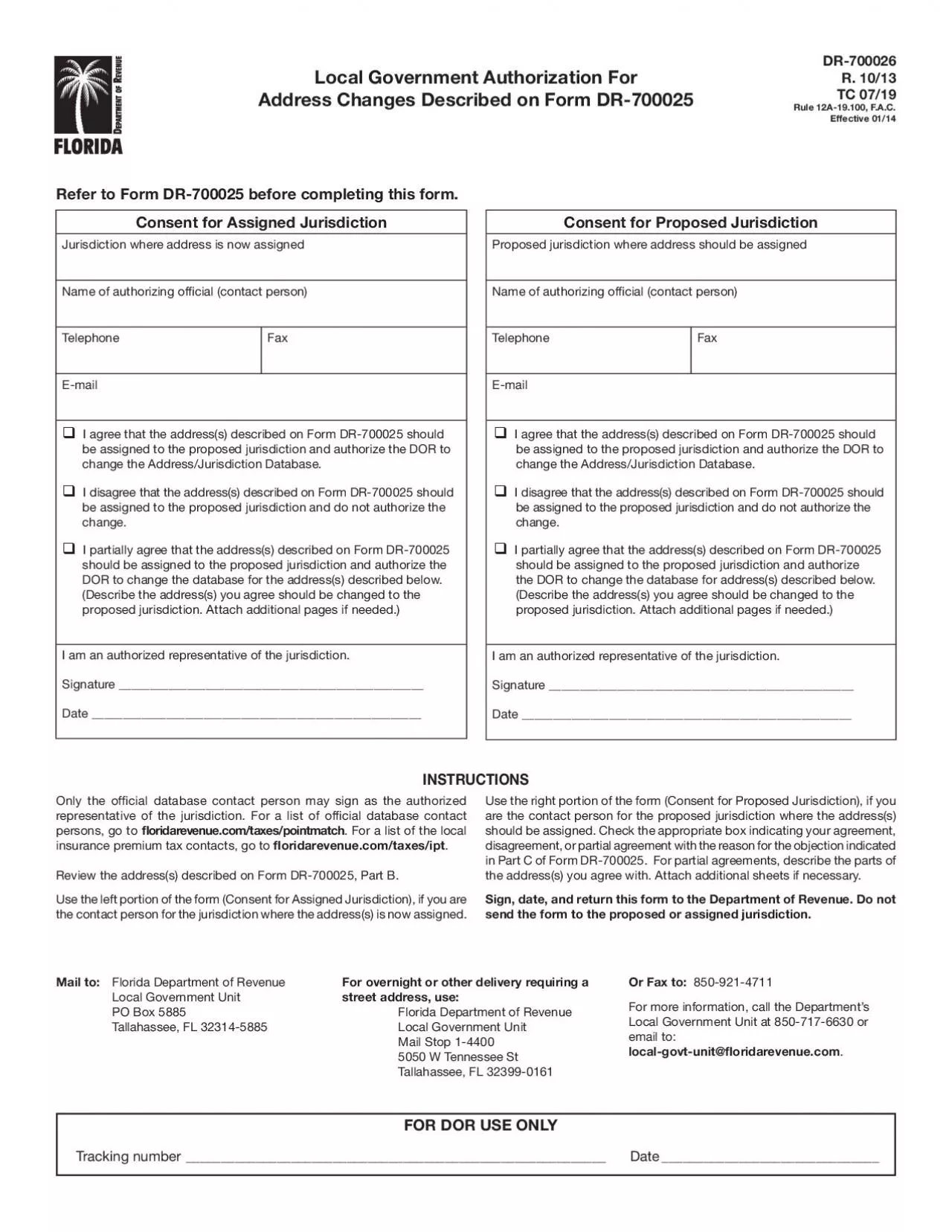
Consent for Proposed JurisdictionProposed jurisdiction where address should be assignedName of authorizing of31cial contact personTelephone FaxEmail I agree that
Download Presentation
"Refer to Form DR700025 before completing this form" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement. Download
Presentation Transcript
Transcript not available.