PPT-1/19/2018 1 1/19/2018 2 Update on Prevention of Cardiovascular Disease in Adults With
Author : ida | Published Date : 2024-02-09
Farzad Hadaegh MD Professor of Internal Medicine amp Endocrinology Prevention of Metabolic Disorders Research Center Research Institute for Endocrine Sciences
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "1/19/2018 1 1/19/2018 2 Update on Preven..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
1/19/2018 1 1/19/2018 2 Update on Prevention of Cardiovascular Disease in Adults With: Transcript
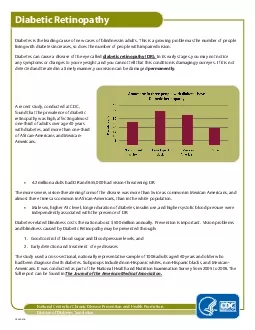
Farzad Hadaegh MD Professor of Internal Medicine amp Endocrinology Prevention of Metabolic Disorders Research Center Research Institute for Endocrine Sciences Shahid Beheshti University of Medical Sciences . By: Jeremy Clark, Megan Windland, and Tiana Nater. Negative Effects of Cardiovascular disease. Eating foods that are high in saturated fats and cholesterol may cause plaque to form on artery walls. . PredictingHeart AttackandStroke risk Prevention of Cardiovascular DiseasePocket Guidelines for Assessment and Management of Cardiovascular Risk (WHO/ISH Cardiovascular Risk Prediction Charts for WHO e Prevention & Treatment. . in Women: Update on the . 2011 American Heart Association Guidelines. Objectives. Discuss strategies to assess and stratify women into high risk, at risk, and ideal health categories for cardiovascular disease (CVD). Toni . Mustahsani. . Aprami. , dr., . Sp.PD. , Sp.JP. Department of Cardiology and Vascular Medicine. Cardiovascular Subdivision, Department of Internal Medicine. Hasan. . Sadikin. Hospital/Medical School, . Slide 1: . Target. population/question. 2. 09/01/2018. Patients with inflammatory joint disorders, particularly rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis. To update the EULAR 2009 cardiovascular disease (. Dr. Gabriel S. Tajeu, DrPH, MPH. NIH T-32 Postdoctoral Fellow: . Vascular Biology and Hypertension. University . of Alabama at . Birmingham. No disclosures. Project . support by NIH/NHBLI . T32HL007457-34. Division of Diabetes TranslationRule of thirds GuidesRule of thirds GuidesDiabet Retinopathy Diabetes is the leading cause of new cases of blindness in adults This is a growing problem as the number This brochure is designed to help public health program planners community Introduce clinical decision-support systems within healthcare systems to implement clinical guidelines at the point of care R Contents of this PresentationChapters in the 2021 Statistical UpdateSlide 3Key InformationSlide 4What’s New OverallSlide 10New dataSlide 11Additional ResourcesSlide 12 2021 Statistical Update Cha 1 Cardiovascular Disease in Virginia Cardiovascular disease is the most common cause of acute and chronic illness globally, in the U.S. and in Virginia. Affecting the heart and blood vessels, cardio Jan - March 201 8 ; 5 ( 1 ): 2 3 - 2 9 Page 23 www.ijmse.com International Journal of Medical Science and Education An official Publication of Association for Scientific and Medical Education (ASME Anne B. Newman, MD, MPH. Professor of Epidemiology and Medicine. University of Pittsburgh. Cardiovascular disease is disabling. Disability (. Ettinger. 1993). H. eart disease = 15% of men and 10% of women . A 2023 Presidential Advisory From the AHA. Definition of . Cardiovascular-Kidney-Metabolic Syndrome (CKM). A systemic disorder characterized by pathophysiologic interactions among metabolic risk factors, chronic kidney disease, and the cardiovascular system, leading to multi-organ dysfunction and a high rate of adverse cardiovascular outcomes.. A Scientific Statement From the AHA. Definition of . Cardiovascular-Kidney-Metabolic Syndrome (CKM). A systemic disorder characterized by pathophysiologic interactions among metabolic risk factors, chronic kidney disease, and the cardiovascular system, leading to multi-organ dysfunction and a high rate of adverse cardiovascular outcomes..
Download Document
Here is the link to download the presentation.
"1/19/2018 1 1/19/2018 2 Update on Prevention of Cardiovascular Disease in Adults With"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents