PPT-Pancreatic Tumours Ass.
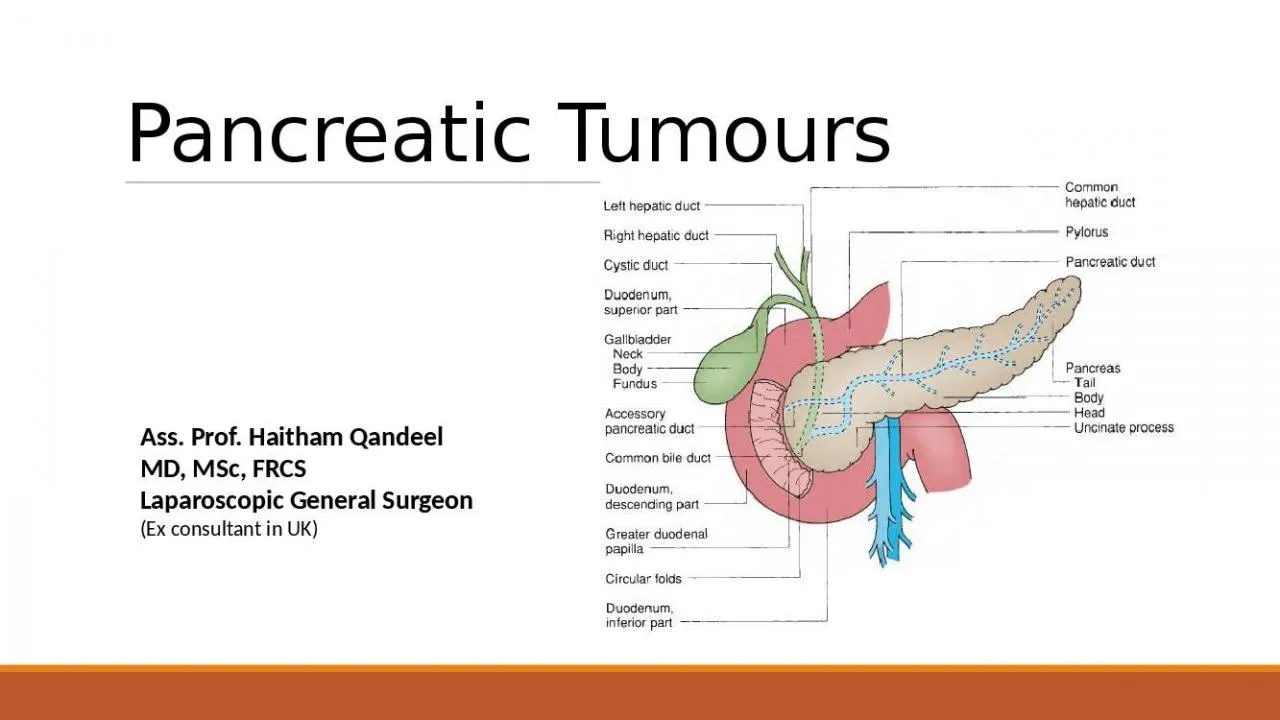
Prof Haitham Qandeel MD MSc FRCS Laparoscopic General Surgeon Ex consultant in UK STRUCTURE AND HISTOLOGY The pancreas has two major components the exocrine structure
Download Presentation
"Pancreatic Tumours Ass." is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement. Download
Presentation Transcript
Transcript not available.