PDF-Antibiotics Anti
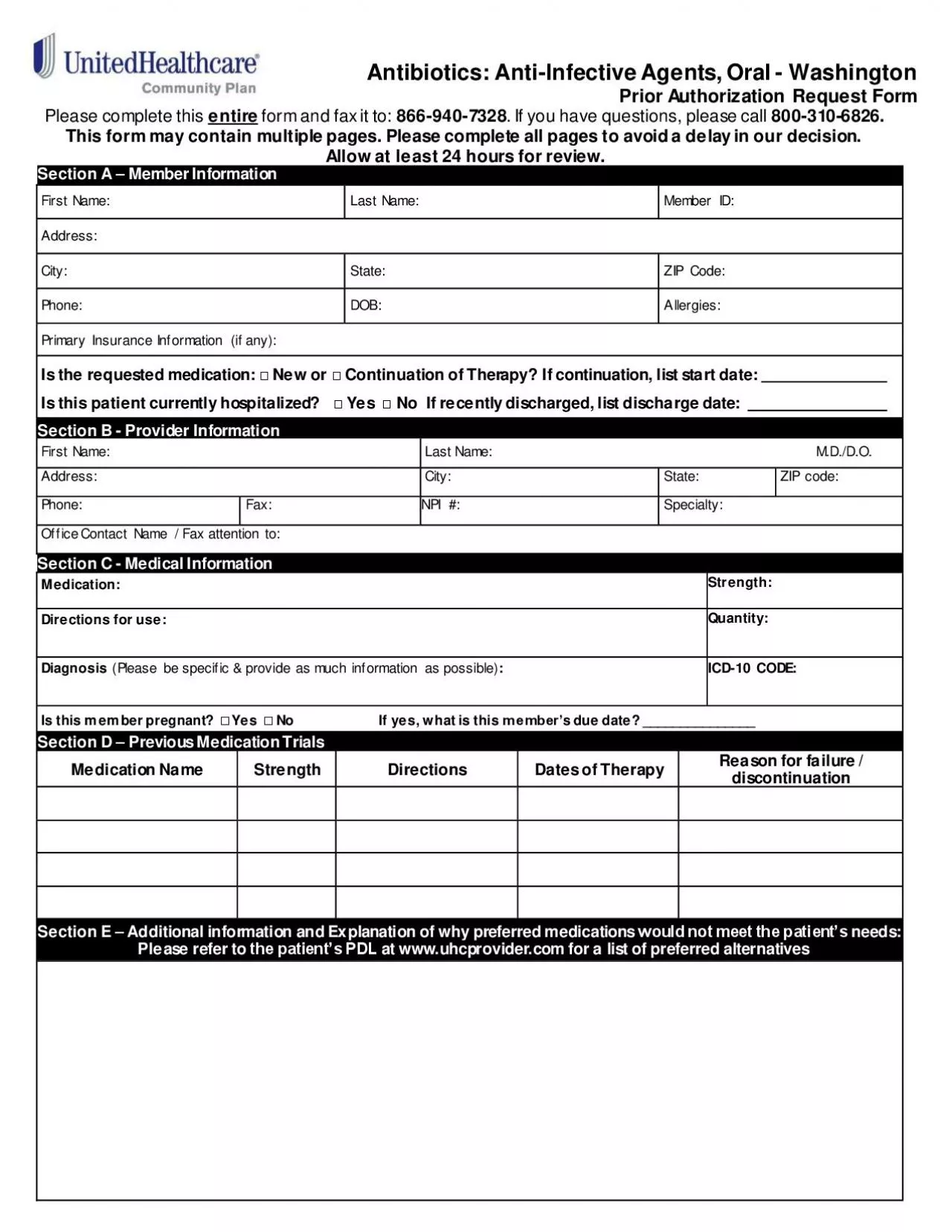
Infective Agents Oral Washington
Prior Authorization Request Form
Please complete this entire
form and fax it to
866 940 7328 If you have questions please call 800
Download Presentation
"Antibiotics Anti" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement. Download
Presentation Transcript
Transcript not available.