Explore
Featured
Recent
Articles
Topics
Login
Upload
Featured
Recent
Articles
Topics
Login
Upload
Search Results for 'Zip-Certify'
Zip-Certify published presentations and documents on DocSlides.
Zip Line Kits For Kids
by buyziplinekitsnow
We specialize in large selection of backyard zip l...
Backyard Zip Line
by buyziplinekitsnow
http://www.buyziplinekitsnow.com buyziplinekitsno...
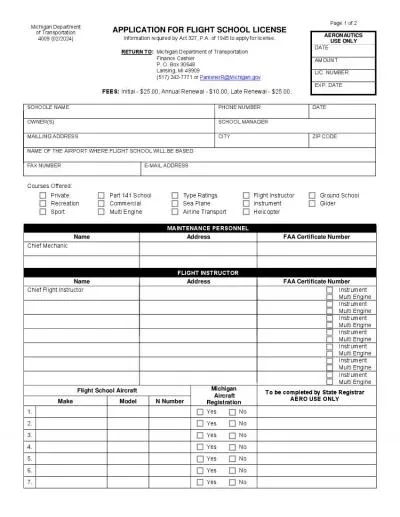
Michigan Department of State
by white
Notice of Rejection of Vehicle Financing Vehicle I...
Effort Reporting How to Certify Effort in Employee Compensation Compliance ECC
by victoria
How Do I Know When To Certify?. UMass Dartmouth ce...
23 certify that given above the anAbelief.
by mentegor
Distric 162 81 Distric 100 204 Stat Oi For Revise ...
Recognition of Foreign Certifying Authorities
by conchita-marotz
Vakul Sharma. © Vakul Corporate Advisory, 2014. ...
Zip Code Day 6-14-14 Zip Code Day
by aaron
6-14-14. Celebrate Zip Code Day. With Us in . Alt...
I certify the applicant is print handicapped as indicated above Secti
by delilah
WEYE Seeing Eye Radio of Goodwill Industries of Ak...
Vendor Identification Codes, Zip Codes, 1099s and Unclaimed Property
by bery
Sylvia James. Director of Fiscal Services. Budget,...
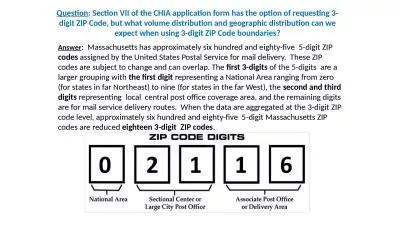
Question : Section VII of the CHIA application form has the option of requesting 3-digit ZIP Code,
by miller
Answer. : Massachusetts has approximately six hun...
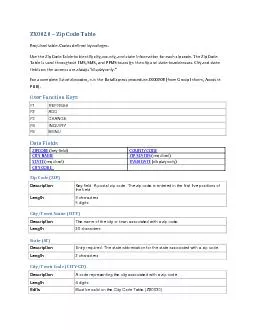
ZX0020 Zip Code TableRequired table Codes defined by colleges Use th
by tremblay
F1 REFRESH F2 ADD F3 CHANGE F4 INQUIRY F8 MENU Dat...
How to Extract / UnRAR with 7-Zip
by shangmaxi
(This version is made for windows Vista). Most of ...
3.Zippo : Moon Landing
by marina-yarberry
3.Zippo : Moon Landing 4.Zippo: The Revel...
Zip Code Lookup Market Analysis
by stefany-barnette
Zip Code Lookup Market Analysis What is a market ...
Zip Code Lookup Market Analysis
by pasty-toler
Zip Code Lookup Market Analysis What is a market ...
Zip L ine Physics A Challenge Based Design Unit
by aaron
Zip L ine Physics A Challenge Based Design Unit ...
Zipping Up Comfort Fiep , Judith, Roos, Braden, and Sam
by tawny-fly
What we are doing. Helping the Autism, anxiety, a...
4 .Zippo: BELLE KOGAN (1939)
by kittie-lecroy
5. .Zippo: . LEATHER (1951) . 6. .Zippo: . 80th A...
Missouri ZIP Code Health Rankings
by cheryl-pisano
Stephen Njenga, Director of Performance Measureme...
The Zipper
by danika-pritchard
By: Chris Henry. What is a Wedge?. A . wedge is a...
FÓRMULA DE ZIPF: UN ESTUDIO SOBRE SU APARICIÓN EN DIVERS
by tatiana-dople
EVA MARÍA GIL CENTENO , DESIRÉE MORENO POZO. P...
The Zipper Slipper
by karlyn-bohler
June K.. 12. Virginia. Have a great idea fo...
Generic Name For Ziprasidone
by faustina-dinatale
cheap geodon online. generic geodon cheap. buy ge...
The Zipper Fixer
by debby-jeon
Kyra M.. 8 years old . Mississippi , USA . Step 1...
HIGH SCHOOLGED INFORMATION SchoolAgency City State Zip CEEB Code Graduation Date Tech Prep Student Yes No COLLEGES ATTENDED College Name City State Zip College Name City State Zip College Name City
by alexa-scheidler
Intent to Apply for Financial Aid and Complete th...
Open the Zipper.
by trish-goza
2 Zipper: Center and layer the Zipper on the rig...
Zippo Manufacturing Company
by stefany-barnette
Power of the Zippo Brand. After . nearly 80 years...
THE ZIPPER
by tatiana-dople
A . mechanical. . prodigy. Blanca Fernández Her...
1 Zippy Shell Mobile Storage Systems was
by celsa-spraggs
launched in Australia in 2007. After several year...
Hand Surgery Certifying Examination
by certsgotlearning
#Certification #Dumps #Certification_exam_Dumps
SCC Certifying Examination
by certsgotlearning
#Certification #Dumps #Certification_exam_Dumps
Pediatric Surgery Certifying Examination
by certsgotlearning
#Certification #Dumps #Certification_exam_Dumps
Vascular Surgery Certifying Examination
by certsgotlearning
#Certification #Dumps #Certification_exam_Dumps
General Surgery Certifying Examination (CE)
by certsgotlearning
#Certification #Dumps #Certification_exam_Dumps
hMAhx00660074chOddbhh
by okelly
MPaUhhdahhenclosed Michigan Have a agreement with ...
Type or print your Full NameYour Social Security NumberHome Address 15
by olivia
I elect an Arizona withholding percentage of zero ...
CLEAR FORM
by paisley
Services Site. GEFENSE IOGHSTHFSBATTIE FREEK,MHFHH...
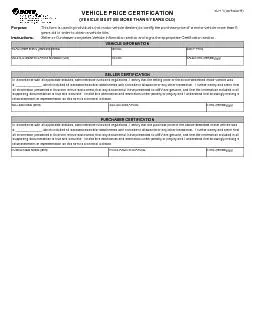
In accordance with all applicable statutes administrative rules and r
by beatrice
PURCHASER CERTIFICATION PURCHASER NAME (print) PUR...
North Carolina National Guard
by eddey
Education Ser vices Office Phone Number: (984) 664...
Gettysbur
by ceila
Distric I 162 81 100 122 Stat For
Load More...