PPT-Cough: A workshop highlighting two new GP guidelines on
Author : sherrill-nordquist | Published Date : 2020-01-29
Cough A workshop highlighting two new GP guidelines on the Investigation of symptoms of lung cancer and Chronic Obstructive Pulmonary Disease Gold Coast Arts Centre
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Cough: A workshop highlighting two new G..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Cough: A workshop highlighting two new GP guidelines on: Transcript
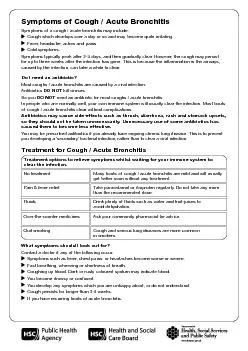
Cough A workshop highlighting two new GP guidelines on the Investigation of symptoms of lung cancer and Chronic Obstructive Pulmonary Disease Gold Coast Arts Centre 21 May 2014 Dr Siva P Sivakumaran. The First Data FD100 terminal combines performance, security and ease of use plus adaptability when your processing needs change. A different paradigm has evolved in which cough is viewed as the primary condition characterised by afferent neuronal hypersensitivity and different aspects of this syndrome are manifest in the different phenotypes of cough There are several advanta Cough which develops over a day or so and may become quite irritating. Fever, headache, aches and pains. Cold symptoms.Symptoms typically peak after 2-3 days, and then gradually clear. However, the Baz. Lazar . SLIME 14. th. October 2013. Overview. Definition and causes. Finals Clinical Case – work through. History and examination. Management. Information sheet. 5 things about ILD. Chronic disease, often idiopathic. What’s All The Whoop About. What is Pertussis. Bordetella. pertussis . also referred to as . Whooping Cough. Whooping cough is a disease caused by a fastidious pathogen that invades the respiratory system. This pathogen secretes a toxin that disrupts the normal function of cilia in the lungs, resulting in a severe cough.. http://www.naatw.org. File Edit View History Bookmark Window Help. Search. Insert your bookmarks here News Web. 2016 Guidelines Workshop. @NAATW 2016. E-mail. : info@naatw.org http://www.naatw.org. Cough associated with an upper respiratory tract infection is generally treated with medicines that are available without prescription, but there is . disagreement about their effectiveness. .. There can be little doubt of the faith of the general public in non-prescription cough treatments, with a total of more than 80 proprietary brands and variants on the market and . Working together to protect teens. Rx and OTC Medicine Abuse. The Office of National Drug Control Policy reports that medicine abuse is our nation’s . fastest-growing. . drug problem. . Teens Turn to Medicine Cabinets to Get High. Cold and cough become a reason for worry when the symptoms involve a running nose, a blocked and stuffy nose making breathing difficult, cough that disrupts the sleep and even more so when it is accompanied with fever. Purpose To identify active cases of Tuberculosis TB before it can spread in homeless shelter detoxification facilities and other congregate group settingsBackgroundCongregate settings such as homeless ASSO.PROF.PEDIATRICS. ICH,GOVT MEDICAL COLLEGE,KOTTAYAM. LEARNING OBJECTIVES. To write 2 agents causing whoop like cough. To list 2 clinical features of whooping cough. To name 3 complication of whooping cough. Department of . Pharmacology. JNMC, AMU. . INTRODUCTION. D. efensive reflex . that . enhances. clearance . of secretions and . particulates from airways . Provides protection . from aspiration . of foreign materials. Jodi Allen (Senior Speech and Language Therapist). Jodi.allen@nhs.net. . @. JodiAllenSLT. The National Hospital for Neurology and Neurosurgery, Queen Square, London, WC1N 3BG. Disclosures . No disclosures. MSc in clinical pharmacy. Coughing is a protective reflex action caused when the airway is being irritated or obstructed. Its purpose is to clear the airway so that breathing can continue normally..
Download Document
Here is the link to download the presentation.
"Cough: A workshop highlighting two new GP guidelines on"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents