PPT-SCABIES
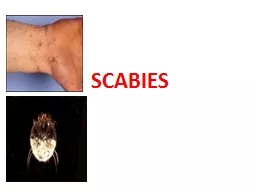
Causative organism scabies mite sarcoptes scabei var hominis an obligate human parasite Animal scabies mites may result in transient symptoms in humans but they
Download Presentation
"SCABIES" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.