PPT-The lacrimal system Eslam shamailah
Author : carny | Published Date : 2024-01-03
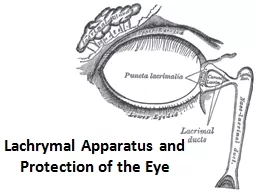
Naba jehad Dania Al Tarawneh Anatomy Introduction Disorders of the lacrimal system are common and may produce chronic symptoms with a significant morbidity The
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "The lacrimal system Eslam shamailah" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
The lacrimal system Eslam shamailah: Transcript
Download Rules Of Document
"The lacrimal system Eslam shamailah"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents