PPT-Reduce Waste and Improve Outcomes
Author : kittie-lecroy | Published Date : 2018-11-07
Darilyn V Moyer MD FACP Chair ACP Board of Governors Disclosures Elected Chair of BOG Not specifically asked to speak about MOC Learning Objectives Define High Value
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Reduce Waste and Improve Outcomes" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Reduce Waste and Improve Outcomes: Transcript
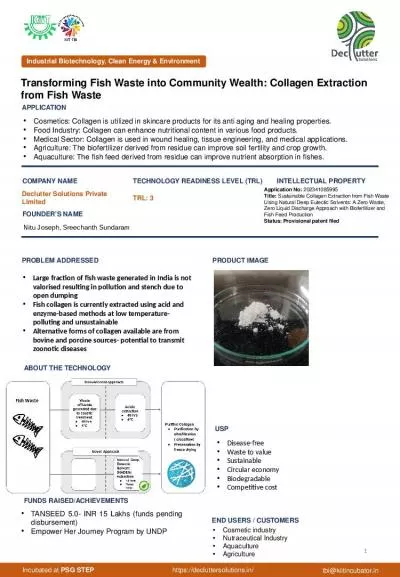
Darilyn V Moyer MD FACP Chair ACP Board of Governors Disclosures Elected Chair of BOG Not specifically asked to speak about MOC Learning Objectives Define High Value Care Utilize the High Value Care Curriculum and Cases . Richard Swannell. WRAP. Introduction. Why develop guidance?. What does it contain?. Conclusions and next steps.. Why?. To support the Save Food initiative. To help Governments, Municipalities and businesses to drive change. 1. 1.03 B UNDERSTAND. REDUCE, REUSE, RECYCLE. The best place to practice conserving resources is at home. Individuals can substantially. REDUCE, REUSE, AND RECYCLE . waste and conserving resources by practicing the following. Tutorial . on . the . Essential Version . of the Health IT-enabled Quality Improvement (. eCQI. ) . Worksheet. Welcome!. Hello, my name is Ellen. I’m going to share a tool . that . will help you . You will feel great about helping the earth by reducing the garbage you throw away.. To keep your school . yard . cleaner . and . free from . litter. .. A waste-free lunch is often healthier!. Saves YOU and your parents money because a waste-free lunch often costs less.. U.S DOT Hazmat Training . DOT Hazmat Training Requirements. Training must be completed within 90 days of employment . Employee can perform Hazmat functions (until trained) if directly supervised. Retraining is required every three years. Patients do . not. take their medicine . as prescribed. about . half. the time. . 2. Why is it important to assess adherence?. =. 3. 4. Eight. . steps to . improve medication adherence. in . your. Photo Source. : Justin Sewell. 32%. 24%. of global food supply by weight. A significant share of food intended for human consumption is lost or wasted from the farm to the fork. of global food supply by energy content (calories). Medical Waste Management Market report provides the future growth trend of the market based on in-depth research by industry experts.The global and regional market share along with market drivers and restraints are covered in the report. View More @ https://www.valuemarketresearch.com/report/medical-waste-management-market Focusing on Triglycerides. Primary and Secondary CVD Prevention Trials: . Evaluating Treatment of Triglycerides. Why Have Outcomes Trials of TG-Lowering Drugs Failed to Reach Primary Endpoints? . ASCEND . 1. Word Count Example. We have a large file of words, one word to a line. Count the number of times each distinct word appears in the file. Sample application: analyze web server logs to find popular URLs. Waste and rubbish. Waste management is . understanding what your businesses can control. Types of waste . Members Buy-in - Talk with members . Do they want help. What areas do they want help in (recycling, reducing costs etc) . It is thought that approximately 50% of the food wasted . is . still edible. . The cost of food waste is significant – estimates show that it costs an average family £700 per year.. Source: . Love Food Hate Waste. It is defined as. Waste (also known as rubbish, trash, refuse, garbage, junk) is any unwanted or useless materials.. OR. Any materials unused and rejected as worthless or unwanted and “A useless or profile less activity using or expanding or consuming thoughtlessly or carefully.”. APPLICATION. COMPANY NAME. TECHNOLOGY READINESS LEVEL (TRL). TRL: 3 . INTELLECTUAL PROPERTY . PROBLEM ADDRESSED. ABOUT THE TECHNOLOGY. PRODUCT IMAGE. FUNDS RAISED/ACHIEVEMENTS. TANSEED 5.0- INR 15 Lakhs (funds pending disbursement).
Download Document
Here is the link to download the presentation.
"Reduce Waste and Improve Outcomes"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents