PDF-2. Skin may appear yellowish and, as a result of dehydration, be very
Author : yoshiko-marsland | Published Date : 2016-10-16
Download the PowerPoint presentation from the 2. Skin may appear yellowish and, as a result of dehydration, be very
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "2. Skin may appear yellowish and, as a r..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
2. Skin may appear yellowish and, as a result of dehydration, be very: Transcript
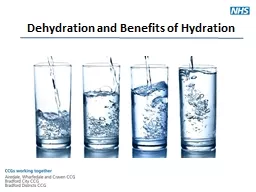
. Very Tasks asymmetrical lumbar pad adjusts up or down to fit with the small of your back while the side independent paddles adjust the level of support Very Task Asymmetrical Lumbar Very Task D Arms Very Tasks optional four dimensional arms offer People with skin picking disorder can and often do have other psychological symptoms like depressio n and anxiety Do all people who pick their skin have skin picking disorder No Research has shown that many people pick at the ir skin from time to t A guide for parents’ and coaches’. . Jennifer Smith. Dehydration. Dehydration occurs when the amount of water leaving the body is more than the amount that it being taken in.. When children exercise they sweat which is an easy way for them to loose water and other essentials that the body needs.. Thirst is first. Thirst is a warning that you are already dehydrated. Dark yellow-orange urine is another . sign. Urine should be a clear, light color unless. You’ve been taking medicine or eating foods that add color. DEHYDRATION . IN . CHILDREN. INTRODUCTION. Children . are particularly susceptible to dehydration with acute. . gastroenteritis or other illnesses that cause . vomiting. , . diarrhoea. . and . BY. Dr. S. E. NWIZU. Consultant . Paediatrician. . Premier Specialists’ Med. Centre.. OUTLINE. INTRODUCTION. BASIC FLUID AND ELECTROLYTE THERAPY. DEHYDRATION. ELECTROLYTE PROBLEMS. INTRODUCTION. Distribution of fluids and electrolytes:. Dehydrating provides us with a connection between cooked and raw foods. It is a method of preservation that helps retain food enzymes and nutrients. The process removes enough water to prevent growth of bacteria, yeast and mold.. Pages 52-53. LESSON PURPOSE. To identify to the student the common signs and symptoms of dehydration, hyponatremia and heat related issues. . PERFORMANCE OBJECTIVES. List the five symptoms which are common to dehydration. . Let’s review: . What are the 4 macromolecules of life?. Let’s Review . 2. What are the monomers of each macromolecule?. 3. What are the polymers of of each macromolecules. 4. Predict: How do you think we go from monomer to polymer?. . Analysis. . Black Pearl 24k Power Point. . Material. Black Pearl 24k Skin Analysis Questions. Black Pearl 24k Skin Analysis . Memo to follow after assessment. BLACK PEARL . 24K Reading Material to accompany Video. Are you looking for hydration drinks to reverse the symptoms of dehydration? This article provides an overview of the 7 best drinks for dehydration! What is Dehydration? . ‘the loss of water or body fluids from an . individual’ . (World Health Organisation 2002) . Dehydration can affect both our physical and . . mental health . It can affect your mood and . p.32. How Are Organic Compounds Formed?. Monomers . = building blocks (units). Polymers . = a larger molecule made of repeating subunits. Monomers link together to form polymers.. Many small molecules. By . Dr. Hussein . AlNaji. Alopecia And . Hypotrichosis. Etiology. Alopecia and . hypotrichosis. are defined as lack of hair in any quantity on a normally haired body surface.. In contrast to . alopecia,.
Download Document
Here is the link to download the presentation.
"2. Skin may appear yellowish and, as a result of dehydration, be very"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents