PDF-HSP nephritis
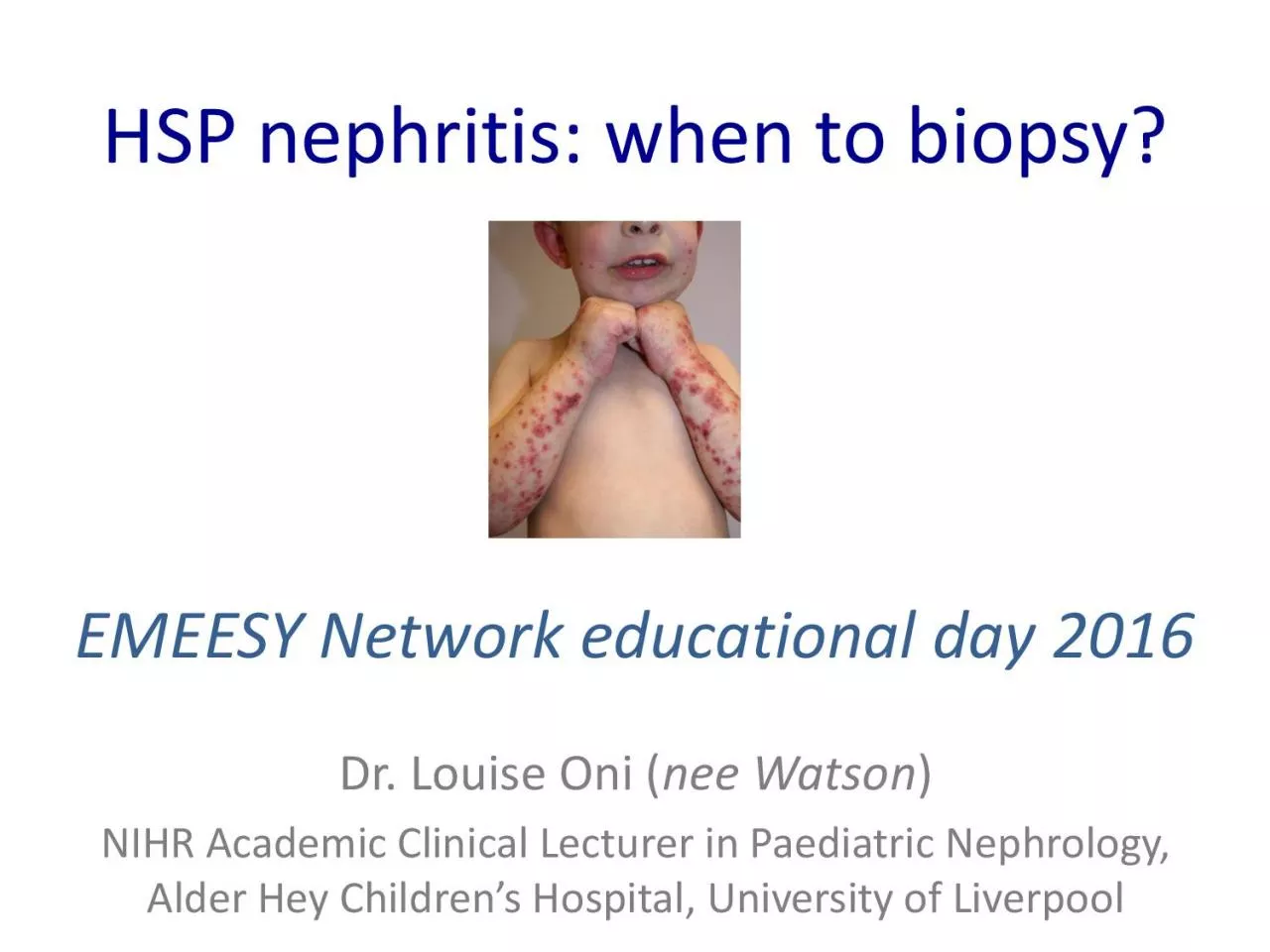
when to biopsy
EMEESY Network educational day 2016
Dr Louise Oni nee Watson NIHR Academic Clinical Lecturer in Paediatric Nephrology Alder Hey Childrens Hospital
Download Presentation
"HSP nephritis" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.